PSC
& PBC
Primary sclerosing cholangitis (PSC) and primary biliary cholangitis (PBC) are diseases of the bile ducts with similar names, but despite sharing certain characteristics and symptoms, they require different treatments and monitoring.

Why it’s important to understand
the difference between PSC and PBC
We have witnessed errors caused by the similarities in the names of the two diseases. We encourage you and your care providers to know the differences between the two diseases. PSC Partners and PSC Support in the United Kingdom have worked with hepatologists who recognize the importance of educating our patients about this issue.
01
PSC and PBC sound like the same disease.
02
Focusing solely on the names of these conditions, both are “primary” diseases (not secondary, meaning, not caused by another condition).
03
Both are “biliary,” diseases of the bile ducts.
04
Following the name change for PBC, both are now characterized by the term “cholangitis.”
05
Despite sharing certain characteristics and symptoms, each condition creates different needs among patients and requires different treatments and monitoring.
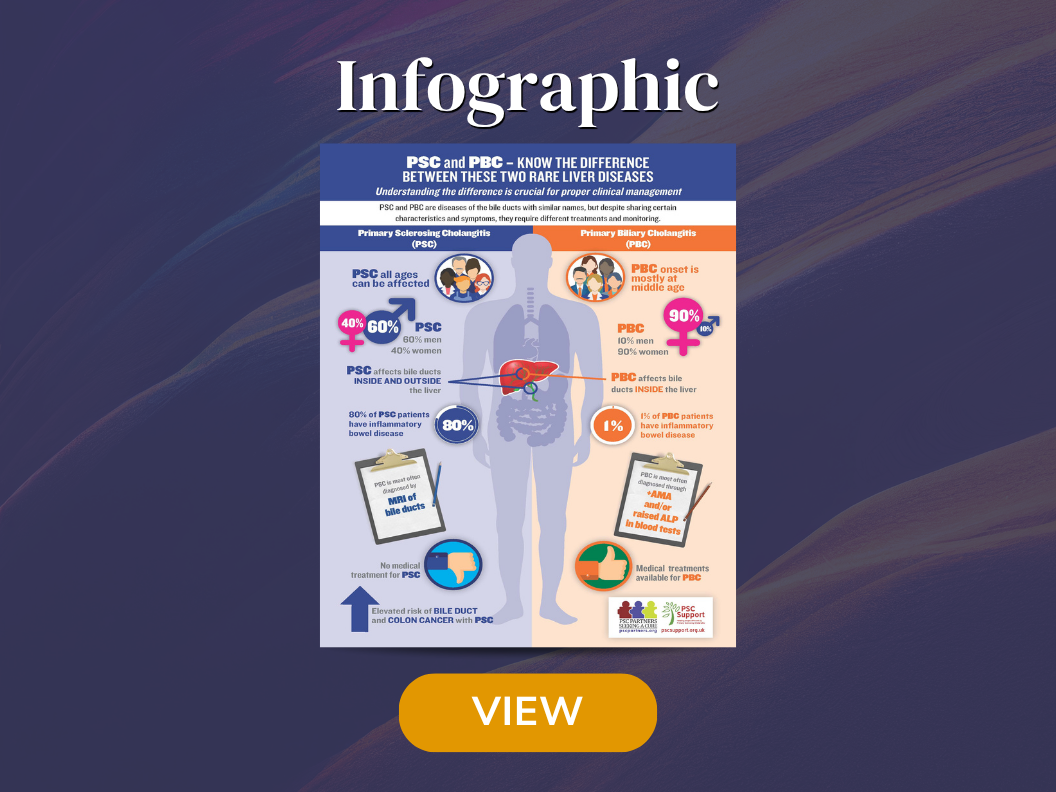
Two Rare Liver Diseases
This printable infographic breaks down PSC and PBC in a simple side-by-side format, making it easier to understand how these similar-sounding conditions differ.
Critical Points
of Difference
The most critical points that distinguish PSC from PBC are presented in the table below.
01
One significant difference between the two diseases is that PSC is considered a premalignant disease, which presents an increased risk of colon and bile duct cancers. Accordingly, PSC patients need to be closely monitored for cancer and for assessing their response to ursodeoxycholic acid (UDCA). PBC has no such increased risks. An erroneous diagnosis that results in neglect of regular monitoring could have disastrous results for PSC patients.
02
A second difference between PSC and PBC is how the two diseases manifest in patients. PSC affects individual patients differently; there is no single disease course, and many factors need to be considered with PSC. PSC has several unknowns and many unmet needs, but PBC is not as multilayered.
03
Furthermore, the World Health Organization (WHO) classifies and provides different codes for each disease. PSC and PBC may be confused in disease coding for insurance or for medication purposes. Whether you are a patient or a caregiver, please ensure you know the potential for error. The ICD-10-CM Code for PSC is K83.01.
Similarities and differences between PSC and PBC
| FEATURE | PSC – PRIMARY SCLEROSING CHOLANGITIS | PBC – PRIMARY BILIARY CHOLANGITIS (COMMONLY STILL REFERRED TO AS PRIMARY BILIARY CIRRHOSIS) |
|---|---|---|
| Site of disease involvement | Bile ducts inside and outside the liver; however in small duct PSC (10-15% of patients) only the small ducts inside the liver are affected | Small bile ducts inside the liver only |
| Mode of diagnosis | Usually by MRI of bile ducts. Occasionally liver biopsy or ERCP is needed | Two of the following: Raised ALP, positive disease specific antibodies (AMA), diagnostic liver biopsy. |
| Associated with increased risk of bile duct cancer and colon cancer | Yes | No |
| Response to ursodeoxycholic acid (UDCA) | Improves liver blood tests in some patients; not conclusively proven to slow disease progression | Associated with improved prognosis in those individuals who respond well to UDCA |
| Co-existing inflammatory bowel disease (IBD) | Around 80% of patients have IBD – mostly colitis | Very rare and not characteristic; around 1% |
| Common symptoms in early disease | Itching, fatigue, abdominal pain, cholangitis flares | Itching, fatigue, dry eyes and mouth, abdominal pain |
| Gender predominance | 60% men, 40% women | 90% women, 10% men |
| Average age at diagnosis | Any age; mostly around 40 years | 75% are affected in middle age (>45 years old) |
| Associated with excess alcohol consumption | No | No |
| Associated with smoking history | Most often non-smokers | Associated with a history of smoking |
References and Further Reading
- EASL Clinical Practice Guidelines: management of cholestatic liver diseases. J Hepatol 2009;51:237–67. doi:10.1016/j.jhep.2009.04.009
- Hirschfield GM, Karlsen TH, Lindor KD, et al. Primary sclerosing cholangitis. Lancet 2013;382:1587–99. doi:10.1016/S0140-6736(13)60096-3
- Trivedi PJ, Corpechot C, Pares A, et al. Risk Stratification in autoimmune cholestatic liver diseases: Opportunities for clinicians and trialists. Hepatology 2015;:n/a – n/a. doi:10.1002/hep.28128
- Boonstra K, Weersma RK, van Erpecum KJ, et al. Population-based epidemiology, malignancy risk, and outcome of primary sclerosing cholangitis. Hepatology 2013;58:2045–55. doi:10.1002/hep.26565
- Trivedi PJ, Hirschfield GM. Treatment of autoimmune liver disease: current and future therapeutic options. Ther Adv Chronic Dis 2013;4:119–41. doi:10.1177/2040622313478646
- Hirschfield GM, Gershwin ME. The immunobiology and pathophysiology of primary biliary cirrhosis. Annu Rev Pathol2013;8:303–30. doi:10.1146/annurev-pathol-020712-164014
- Floreani A, Franceschet I, Cazzagon N, et al. Extrahepatic autoimmune conditions associated with primary biliary cirrhosis. Clin Rev Allergy Immunol 2015;48:192–7. doi:10.1007/s12016-014-8427-x
- Corpechot C, Gaouar F, Chrétien Y, et al. Smoking as an independent risk factor of liver fibrosis in primary biliary cirrhosis. J Hepatol. 2012 Jan;56(1):218-24. doi: 10.1016/j.jhep.2011.03.031. Epub 2011 May 19.
- Juran BD, Lazaridis KN. Environmental factors in primary biliary cirrhosis. Semin Liver Dis. 2014 Aug;34(3):265-72. doi: 10.1055/s-0034-1383726. Epub 2014 Jul 24.
Acknowledgements
PSC Partners Seeking a Cure and PSC Support would like to thank Professor Gideon Hirschfield and Dr. Palak Trivedi for their involvement in helping us provide the following concise comparison between PSC and PBC.
Gideon Hirschfield, Professor/Consultant Hepatologist University of Birmingham/University Hospitals Birmingham
Dr. Palak Trivedi, Academic Clinical Lecturer and SPR in Hepatology and Gastroenterology NIHR Centre for Liver Research; University of Birmingham
FAQ
- PBC patients have justifiably wanted to change the disease name to avoid the stigma of the term cirrhosis.
- By changing cirrhosis to cholangitis, there is no longer a misconception that PBC is caused by alcohol overuse.
- Additionally, 80 percent of PBC patients no longer progress to cirrhosis.
- Unlike most PSC patients, a large number of PBC patients respond to ursodeoxycholic acid (UDCA), which, in their case, slows down disease progression.
- The term cirrhosis in the disease name no longer reflects the reality of the disease.
Experienced hepatologists do not always treat PSC patients. As we know, some gastroenterologists and primary care physicians may never have treated a PSC patient and do not know the risks associated with PSC. In many cases, a patient with a rare disease like PSC will not have access to a hepatologist specializing in PSC or involved in PSC research. Knowing the difference between the two diseases is important because PSC and PBC create different clinical needs.
There are different modes of diagnosis for PSC and for PBC. While the symptoms can be similar, the diseases affect the bile ducts and liver differently and can be distinguished from one another via a combination of blood tests, MRI imaging, and/or liver biopsy.
It is exceedingly rare, but possible, for a person to be diagnosed with both PSC and PBC. This is much rarer than overlap between PSC and other autoimmune diseases, such as autoimmune hepatitis.
Real Progress. Real Stories.
Discover inspiring patient journeys and the latest advances in PSC research.

A Year of Growth, Connection and Momentum
As we step into a new year, we are reflecting on key moments from the past […]
Fight Like Hayley!
I look at my daughter’s picture, a radiant face, a smile so cheerful that it holds no clue of the horrific battle she is still undergoing with PSC.

Caregiving: some do’s and don’ts
No one ever really “plans” to be a caregiver. I know I never thought about it, beyond maybe providing ginger ale and crackers for someone with a stomach bug. But that slowly began to change after I met Nicola over 10 years ago.

Take the First Step
Toward Connection
Stay connected to the PSC community. Get updates on research, events, and stories straight to your inbox.
Subscription Form
"*" indicates required fields